Creating a Health Checkup System for the Elderly in the Kingdom of Bhutan
Sakamoto Ryota
Visiting Associate Professor CSEAS (Hakubi Project)
According to United Nations, at a global level, 5 per cent of the population was at least 65 years of age in 1950 (UN, 2009). By 2009, this proportion had increased to just under 8% (UN ibid). Yet, by 2050, 16% of the world population is projected to be 65 years or over (UN ibid). At present, caring for burgeoning elderly populations is one of the biggest issues being addressed by the international community. According to the Royal Government of Bhutan (RoGB), the number of the aged 65 years or over was 29,745 in 2005 and the number will double by 2030.1 Many adults who survive into late life suffer from high rates of chronic illness and it has been reported that 80% have at least one and 50% have at least two chronic conditions.2 Given the high prevalence and impact of chronic health problems among the elderly, effective and efficient care to address these problems is becoming increasingly important so as to maximize both the quantity and quality of life for the elderly.
Concerned by this situation that affects all of the world’s populations, in May 2009, we started to discuss about ways to care for the elderly in Bhutan with the Ministry of Health (MoH), RoGB, and introduce a health checkup system in the country through a pilot project named “Community Based Medical Care for The Elderly” approved by the Royal Government of Bhutan.3 In October 2010, this resulted in the introduction of a health checkup for the elderly in Khaling, Trashigang Dzongkhag offering us an important opportunity to grasp those problems that the elderly in Bhutan face, and help us consider how to prevent future diseases, disabilities, and avoidable deaths.
The model we employed was Choju Kenshin (長寿健診 Health Checkup for The Elderly) which was first started and employed in Kochi prefecture by Toshio Ozawa, Kozo Matsubayashi and Kiyohito Okumiya. In 1990, they initiated a project entitled Kahoku Longitudinal Aging Study (KLAS) in Kahoku town, Kochi prefecture. Community intervention using their field medical approach contributed not only to improving ADL independence but also suppression of increasing medical care expenses (Matsubayashi et al. 2012). In 1968, James Maxwell Glover Wilson and Gunnar Jungner elaborated the 10 principles of screening for diseases (Table 1) Wilson and Junger 1968).
Table 1. Principles of Early Disease Detection, elaborated by Wilson JMG and Jungner G in 1968
|
1 |
The condition sought should be an important health problem. |
|
2 |
There should be an accepted treatment for patients with recognized diseases. |
|
3 |
Facilities for diagnosis and treatment should be available. |
|
4 |
There should be a recognizable latent or early symptomatic stage. |
|
5 |
There should be a suitable test or examination. |
|
6 |
The test should be acceptable to the population. |
|
7 |
The natural history of the condition, including development from latent to declared disease, should be adequately understood. |
|
8 |
There should be an agreed policy on whom to treat as patients. |
|
9 |
The cost of case-finding (including diagnosis and treatment ofpatients diagnosed) should be economically balanced in relation to possible expenditure on medical care as a whole. |
|
10 |
Case-finding should be a continuing process and not a “onceand for all” project. |
What these conceived principles show is that the items in health checkups must depend and relate to the specific situations of respective communities. In this sense, we have to follow both global evidence and local needs. In Bhutan, through discussion with local people we came to focus on mainly 13 items which we call “5 Ds, I HAVE FUN” for short (See Table 2).
Table 2. Focused Items in Community Based Medical Care for the Elderly in Bhutan (5Ds, I HAVE FUN)
|
1 |
Disability |
|
|
2 |
Dementia |
|
|
3 |
Depression |
|
|
4 |
Diabetes |
|
|
5 |
Dental problem |
|
|
6 |
Isolation |
|
|
7 |
Hypertension |
|
|
8 |
Addiction |
|
|
9 |
Visual Problems |
|
|
10 |
Ear Problems |
|
|
11 |
Falls |
|
|
12 |
Urinary Incontinence |
|
|
13 |
Nutrition |
|
To integrate any project that relates to primary health care, medical staff and villagers understanding is necessary. The Chief Program Officer, Trashigang District Health Officer, and I introduced this project to medical staff in Basic Health Units (BHUs), hospitals, then to village heads, village health workers, and principals in schools. While carrying out this project, we have explained the program to villagers and at the same time, asked them for their opinions. BHU staff asked village leaders to arrange volunteers who would help the checkups. While volunteers were arranged, we would explain about the project and conducted a 2 day training program for them. Afterwards, this facilitated volunteers in carrying out health checkups for the elderly with the support of BHU staff. These checkups were conducted in the houses of elderly who had difficulties in coming to BHU or Outreach Clinics (ORCs).
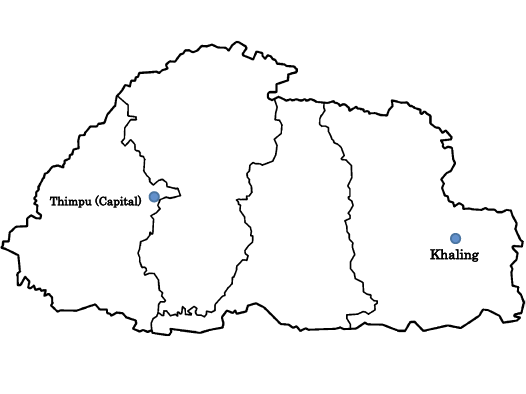
Map of Bhutan

Health checkup for the elderly in Khaling, Bhutan
In total we checked 192 people aged 65 years or over including home visits for 34 people. This meant that we covered almost all the elderly people living in Khaling Gewog covered by Khaling BHU. The mean age for the elderly was 73.8 years among females and 73.0 years among males with the oldest person a lady aged 96 years. Age was determined by a self-enumeration verified with the animal symbols of his/ her birth year. The prevalence of hypertension, obesity, and diabetes were over 71.9%, 6.3%, and 5.7% respectively and what was clear in our field was that impairments to basic activities for daily living increased with aging especially for those over the age of 80 years. Among 30 people who had difficulties in basic activities for daily living, 3 people were suspected to have the after effects of a stroke. 12% of participants had severe hypertension and their systolic blood pressure and diastolic blood pressure were significantly related to their body mass index. The prevalence of diabetes mellitus was 10.8% among the people who were overweight, and 16.7% among those who had obesity. We also visited the homes of the elderly people who had not come to the medical camps and conducted medical checkups. Among those who had not come to the medical camp, 41.2% had difficulties in basic activities for daily living. Quality of Life (QOL) is assessed by using a 100 mm visual analogue scale (lowest QOL on the left end and highest at the right) showed 47.5 for health, 92.0 for family relationships, 83.0 for friendships, 70.0 for economic status and 74.5 for subjective happiness (Sakamoto et al. 2011).

Measuring weight and blood pressure for villagers in Khaling, Bhutan

Elderly cared for by a grandchild in Khaling, Bhutan
 Our main goal is “better health for all” which is the ultimate goal of primary health care. To fulfill this, we include not only people who come to BHUs or ORCs, but also those who do not come to medical facilities. This is because some elderly people cannot come to BHUs or ORCs, even if they want to. For these people, there is a possibility that they may have severe diseases which require care with special attention. Although there are issues of manpower, medical staff should visit the houses of the elderly if and when needed. While in Bhutan, we did not just wait for patients in the hospital, but actively went to villages where we measured weight and blood pressure. While doing so, we explained the importance of weight and blood pressure for protection from stroke and heart attack for as the old adage says, “prevention is better than cure.”
Our main goal is “better health for all” which is the ultimate goal of primary health care. To fulfill this, we include not only people who come to BHUs or ORCs, but also those who do not come to medical facilities. This is because some elderly people cannot come to BHUs or ORCs, even if they want to. For these people, there is a possibility that they may have severe diseases which require care with special attention. Although there are issues of manpower, medical staff should visit the houses of the elderly if and when needed. While in Bhutan, we did not just wait for patients in the hospital, but actively went to villages where we measured weight and blood pressure. While doing so, we explained the importance of weight and blood pressure for protection from stroke and heart attack for as the old adage says, “prevention is better than cure.”
The World Health Organization announced that the leading global risks for mortality in the world are high blood pressure (responsible for 13% of deaths globally), tobacco use (9%), high blood glucose (6%), physical inactivity (6%), and overweight and obesity (5%). These risks are responsible for raising the chance of chronic diseases such as heart disease, diabetes, and various cancers and they affect countries across all income groups: high, middle and low. Eight risk factors (alcohol use, tobacco use, high blood pressure, high body mass index, high cholesterol, high blood glucose, low fruit and vegetable intake, and physical inactivity) account for 61% of cardiovascular deaths. Reducing exposure to these eight risk factors would increase global life expectancy by almost 5 years (WHO 2009). As such, identifying geriatric conditions by performing health checkups can help clinicians manage these conditions and prevent or delay their complications. On the basis of these health checkups, we have tried to promote health of the elderly through comprehensive activities. They should be cared for in collaboration with family, neighbors, village heads, BHUs, hospitals, schools, and so on. While there, we gave a lecture about obesity, hypertension, and diabetes for students of a lower secondary school in cooperation with school teachers.
Between November 7–9, 2011, the first Biennial Health Conference was held in Mongar, Bhutan. MoH, RoGB and adopted a series of recommendations. These acknowledged the impact of pilot project on elderly care which was instituted at Khaling BHU, and recommended to explore the possibility of gradually rolling over the project in the country. It was also recommended to integrate elderly care into the primary health care system during the 11th Five Year Plan. In cooperation with MoH, we are now trying to expand the areas from Khaling to the whole country. Our next aim is to accumulate evidence to support communities through action. We ultimately hope that this elderly program will trigger and help to maintain the bonds and harmony within communities.
References
Centers for Disease Control and Prevention. 2003. Public Health and Aging: Trends in Aging United States and Worldwide. Morbidity and Mortality Weekly Report, 52: 101-106.
Matsubayashi, Kozo and Okumiya, Kiyohito. 2012. Field Medicine: a New Paradigm of Geriatric Medicine. Geriatric Gerontology International, 12: 5-15.
Office of the Census Commissioner, Royal Government of Bhutan. 2005. Results of Population & Housing Census of Bhutan.
Sakamoto, Ryota et al. 2011. Subjective quality of life in older community-dwelling adults in the Kingdom of Bhutan and Japan. Journal of the American Geriatrics Society, 59: 2157-2159.
United Nations. 2009. World Population Ageing. New York: United Nations.
World Health Organization. 2009. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva: WHO Press.
Wilson, James Maxwell Glover and Jungner, Gunnar. 1968. Principles and Practice of Screening for Disease. WHO Chronicle. Geneva: World Health Organization, 22: 473. Public Health Papers 34.
Notes
1 Office of the Census Commissioner, Royal Government of Bhutan. Results of Population & Housing Census of Bhutan 2005.
2 Centers for Disease Control and Prevention. Public health and aging: trends in aging-United States and worldwide. MMWR 2003, 52: 101-106.
3 Project no. GNHC/PMCD-MoH/GEN/ 2010-11/2732